




APAP, should you hit max range (now w/report)


Re: APAP, should you hit you max range
Its fairly commom to place your high end or max pressure approx 2-3 cms above what your 90% pressure was. Its really not a problem to have the max pressure a little high because you'll never reach it if you don't require it.

Re: APAP, should you hit you max range
I rarely hit my maximum pressure. I have my auto set at 10.5 to 13 cm and was last titrated at 11 cm. I spend the majority of my night at 11 cm and just a small portion of the night at 12 cm. My 90% is 12 cm. I only hit 13 cm rarely and that's if I have a mask leak or a "not so good " night for reasons -like stress, eating too close to bedtime, getting to bed late, etc.
If I were hitting 13 every night, I would raise my maximum pressure by at least 1 cm or maybe more. You say you are hitting your maximum of 12 every night. I think you should raise it 1 or 2 cm. It doesn't appear that you need to worry about centrals.
I agree with what several have said - it is the minimum being high enough that is important for optimum therapy.
If you raise your maximum and continue to hit it and your leaks are under control, I would then start raising my minimum pressure slowly, watching the AHI.
If I were hitting 13 every night, I would raise my maximum pressure by at least 1 cm or maybe more. You say you are hitting your maximum of 12 every night. I think you should raise it 1 or 2 cm. It doesn't appear that you need to worry about centrals.
I agree with what several have said - it is the minimum being high enough that is important for optimum therapy.
If you raise your maximum and continue to hit it and your leaks are under control, I would then start raising my minimum pressure slowly, watching the AHI.
_________________
| Machine: DreamStation Auto CPAP Machine |
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Humidifier: DreamStation Heated Humidifier |
| Additional Comments: Backups- FX Nano masks. Backup machine- Airmini auto travel cpap |
-
OldLincoln

- Posts: 779
- Joined: Wed Mar 26, 2008 7:01 pm
- Location: West Coast
Re: APAP, should you hit you max range
My thoughts only: Max is the limit to which pressure may rise. If you have an obstructive apnea that requires more than max to clear, your max setting is too low. The value of the machine is to: 1) prevent events = low setting; and 2) clear events = high setting. It doesn't do any good to have the machine and die of an uncleared apnea because the upper level is too low to clear it.
If you are hitting the high you don't know if the event was cleared by the machine or time. If your pressure chart shows it sticking at the high, not just bump and drop, then you ether had a central that the machine didn't catch or your event needed higher pressure to clear. I have to trust the machine with my life and it is designed to test for a central and back of if it determines that's what it is. However the Max setting is up to me so I let the machine do it's job.
I do not like hitting max high and if I do so more than a couple times a night for a few nights, I'll raise it 2 points.
If you are hitting the high you don't know if the event was cleared by the machine or time. If your pressure chart shows it sticking at the high, not just bump and drop, then you ether had a central that the machine didn't catch or your event needed higher pressure to clear. I have to trust the machine with my life and it is designed to test for a central and back of if it determines that's what it is. However the Max setting is up to me so I let the machine do it's job.
I do not like hitting max high and if I do so more than a couple times a night for a few nights, I'll raise it 2 points.
ResMed AirSense 10 AutoSet / F&P Simplex / DME: VA
It's going to be okay in the end; if it's not okay, it's not the end.
It's going to be okay in the end; if it's not okay, it's not the end.

Re: APAP, should you hit you max range
You had to mention centrals.. I am so afraid of centrals. This is the reason even brought up this subject, I feel I should raise my max to 13 or 14 but I'm afraid of triggering centrals so if what I have now works I will leave it.
Here is a typical night for me:
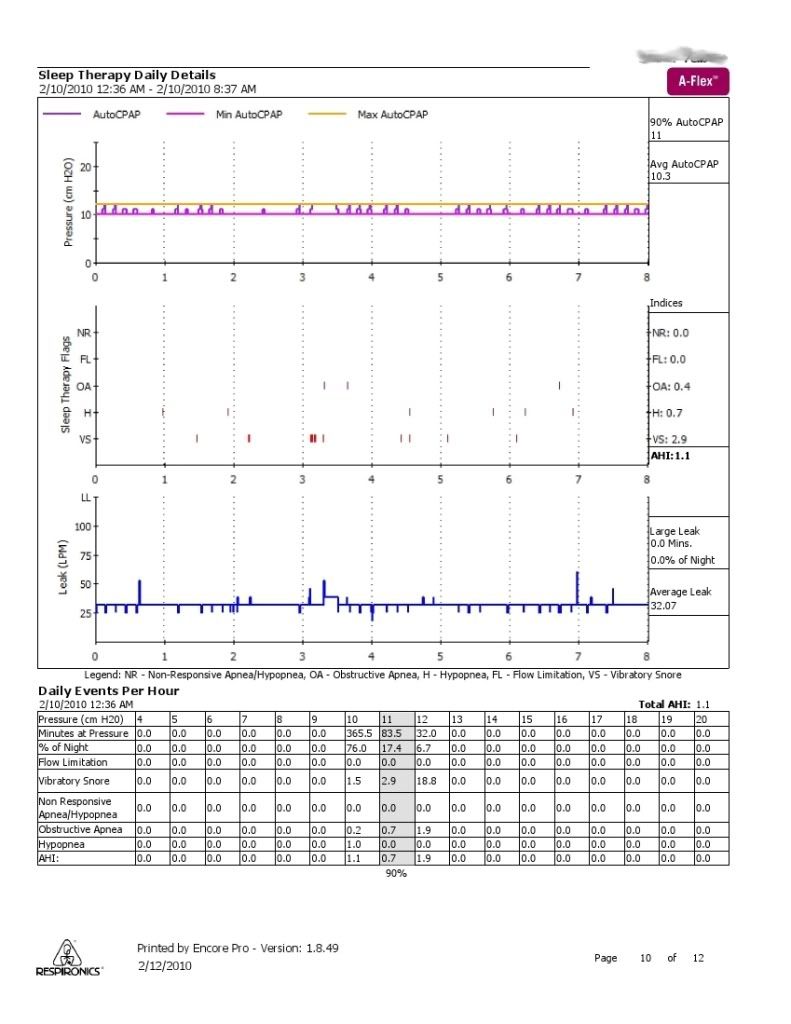
As you can see I had 32 minutes at max, but it is mostly spikes and 90% 11.
So looking at this is 12cm fine or should I raise it? I am now more confused than ever
Here is a typical night for me:
As you can see I had 32 minutes at max, but it is mostly spikes and 90% 11.
So looking at this is 12cm fine or should I raise it? I am now more confused than ever

Re: APAP, should you hit max range (now w/report)
Thanks for posting that report.
My opinion......
You're being needlessly paranoid about Central Apneas.
All those little pressure bumps are unnecessary. For the most part, they're not responding to anything......and can be disturbing to your sleep. You're not even having any Flow Limitations. The area just past the three-hour mark where your pressure went up to 12 was a response to some brief snoring and a very small leak spike.
My recommendation would be to set your machine in CPAP mode at a pressure of 11 cm. for a week or two and see how your reports look (and how you feel).
Although it's not an ideal indicator, the Daily Events Per Hour chart at the bottom shows that you had your best numbers at 11 cm.
Den
My opinion......
You're being needlessly paranoid about Central Apneas.
All those little pressure bumps are unnecessary. For the most part, they're not responding to anything......and can be disturbing to your sleep. You're not even having any Flow Limitations. The area just past the three-hour mark where your pressure went up to 12 was a response to some brief snoring and a very small leak spike.
My recommendation would be to set your machine in CPAP mode at a pressure of 11 cm. for a week or two and see how your reports look (and how you feel).
Although it's not an ideal indicator, the Daily Events Per Hour chart at the bottom shows that you had your best numbers at 11 cm.
Den
(5) REMstar Autos w/C-Flex & (6) REMstar Pro 2 CPAPs w/C-Flex - Pressure Setting = 14 cm.
"Passover" Humidification - ResMed Ultra Mirage FF - Encore Pro w/Card Reader & MyEncore software - Chiroflow pillow
User since 05/14/05
"Passover" Humidification - ResMed Ultra Mirage FF - Encore Pro w/Card Reader & MyEncore software - Chiroflow pillow
User since 05/14/05
-
JohnBFisher

- Posts: 3821
- Joined: Wed Oct 14, 2009 6:33 am
Re: APAP, should you hit you max range
I have to agree with Wulfman on this. Central apneas only impact about 5 to 10 percent of the general population. Pressure induced apneas may only be another 20 percent. The leading cause of central apnea is heart problems. It's a pretty small percentage of those who have central apneas but no heart problems. So, if you are a healthy individual you should not have problems.Imacpaper wrote:... You had to mention centrals.. I am so afraid of centrals. This is the reason even brought up this subject, I feel I should raise my max to 13 or 14 but I'm afraid of triggering centrals so if what I have now works I will leave it. ...
That being said, if an increase in pressure does increase your apneas, you can easily adjust by decreasing your pressure. For all intents and purposes a central apnea will just be another apnea for your body. You will arouse enough (move to a lighter level of sleep) to start breathing. It's REALLY rare for the apnea to be so long that you awaken. It's natural. You just don't want it to go on night after night after night. Then it remains untreated and does the same damage as untreated obstructive apneas.
So, go ahead and try. If you Apnea Hypopnea Index (AHI) increases, drop the pressure.
Hope that helps!
_________________
| Mask: Quattro™ FX Full Face CPAP Mask with Headgear |
| Additional Comments: User of xPAP therapy for over 20 yrs. Resmed & Respironics ASV units with EEP=9cm-14cm H2O; PSmin=4cm H2O; PSmax=15cm H2O; Max=25cm H2O |
"I get up. I walk. I fall down. Meanwhile, I keep dancing” from Rabbi Hillel
"I wish to paint in such a manner as if I were photographing dreams." from Zdzisław Beksiński
"I wish to paint in such a manner as if I were photographing dreams." from Zdzisław Beksiński
Re: APAP, should you hit max range (now w/report)
What could be causing these spikes? I just thought that this is what APAP did.All those little pressure bumps are unnecessary. For the most part, they're not responding to anything
Re: APAP, should you hit max range (now w/report)
Well, yes, it is what the Respironics APAPs do. In my opinion, they can be disturbing to one's sleep and unnecessary unless they're actually responding to valid events.......which most of the ones in your report are not.Imacpaper wrote:What could be causing these spikes? I just thought that this is what APAP did.All those little pressure bumps are unnecessary. For the most part, they're not responding to anything
Here's a partial quote from some years back from one of our forum members "Snoredog" (RIP).......
"......those bumps are the Remstar probing for SDB events looking for improvement to sleep, that is completely normal response from the machine in the absence of events, the autos have had it for some time but it is seen more clearly on the AFlex machine."
Den
(5) REMstar Autos w/C-Flex & (6) REMstar Pro 2 CPAPs w/C-Flex - Pressure Setting = 14 cm.
"Passover" Humidification - ResMed Ultra Mirage FF - Encore Pro w/Card Reader & MyEncore software - Chiroflow pillow
User since 05/14/05
"Passover" Humidification - ResMed Ultra Mirage FF - Encore Pro w/Card Reader & MyEncore software - Chiroflow pillow
User since 05/14/05
-
torontoCPAPguy

- Posts: 1015
- Joined: Mon Dec 28, 2009 11:27 am
- Location: Toronto Ontario/Buffalo NY
Re: APAP, should you hit max range (now w/report)
Although a relative newbie, I am also a techie and from a medical family. I am not a great believer in titration and am a big believer in APAP these days.
I stand to be corrected if I am wrong and always look for education....
My thoughts are simply that titration really depends on a lot of things that are difficult to measure in one night of work. For instance was I sleeping on my side or my back? It makes a difference in pressure requirements. Did I smoosh my nose up against the pillow? What kind of mask was I wearing at the time? It makes a big difference - for example with the Swift LT nasal pillows - as when I smoosh my nose I also smoosh my nasal pillows into my nares and cut the flow of air (i.e. crank up the pressure boss - looks like an obstruction to me). And so on.
I like the APAP machines and am presently using the S8 Autoset II which detects an impending blockage by the 'vibrations' present in the airflow and cranks up the pressure until the vibrations caused by the closing airway cease, thereby avoiding a blockage event and titrating down as low as the pressure can go once again without any impending incidents. What more could one ask for?
I cannot speak to centrals as I am too unfamiliar with them; the above obviously refers to collapse of the airway or impending collapse of the airway. I don't know how my Autoset deals with 'centrals' as of yet because I do not experience them so they are down the list somewhere.
I do know that the Autoset II has provided vastly superior service and performance for me that the basic Escape II CPAP and is much more comfortable overall.
I can also say that looking over the past week of data that my airflow only 'approached' the max end of its range (9 - 15 cm) once... I have no idea why but I am prone to doing wierd things with my mask and hose without thinking.... removing the mask without shutting down the Autoset, having the mask pop off the end of the hose, etc. I intend to reset my data and start afresh tonight. We will see what happens.
I stand to be corrected if I am wrong and always look for education....
My thoughts are simply that titration really depends on a lot of things that are difficult to measure in one night of work. For instance was I sleeping on my side or my back? It makes a difference in pressure requirements. Did I smoosh my nose up against the pillow? What kind of mask was I wearing at the time? It makes a big difference - for example with the Swift LT nasal pillows - as when I smoosh my nose I also smoosh my nasal pillows into my nares and cut the flow of air (i.e. crank up the pressure boss - looks like an obstruction to me). And so on.
I like the APAP machines and am presently using the S8 Autoset II which detects an impending blockage by the 'vibrations' present in the airflow and cranks up the pressure until the vibrations caused by the closing airway cease, thereby avoiding a blockage event and titrating down as low as the pressure can go once again without any impending incidents. What more could one ask for?
I cannot speak to centrals as I am too unfamiliar with them; the above obviously refers to collapse of the airway or impending collapse of the airway. I don't know how my Autoset deals with 'centrals' as of yet because I do not experience them so they are down the list somewhere.
I do know that the Autoset II has provided vastly superior service and performance for me that the basic Escape II CPAP and is much more comfortable overall.
I can also say that looking over the past week of data that my airflow only 'approached' the max end of its range (9 - 15 cm) once... I have no idea why but I am prone to doing wierd things with my mask and hose without thinking.... removing the mask without shutting down the Autoset, having the mask pop off the end of the hose, etc. I intend to reset my data and start afresh tonight. We will see what happens.
_________________
| Mask: Mirage Quattro™ Full Face CPAP Mask with Headgear |
| Humidifier: S9™ Series H5i™ Heated Humidifier with Climate Control |
| Additional Comments: Respironics Everflo Q infusing O2 into APAP line to maintain 95% SaO2; MaxTec Maxflo2 Oxygen Analyzer; Contec CMS50E Recording Pulse Oxymeter |
Fall colours. One of God's gifts. Life is fragile and short, savour every moment no matter what your problems may be. These stunning fall colours from my first outing after surviving a month on life support due to H1N1.

Re: APAP, should you hit you max range
Den, your plan would be such an easy fix! I hear there will be a few empty Senate/House seats available next year, maybe you could go to Washington and take care of that problem along with the economy,healthcare and homeland security!Wulfman wrote:That situation could be fixed by the manufacturers to everyone's monetary benefit.Muse-Inc wrote:I'd had the CPAP for 23 months. They denied my doc's medically necessary switch to APAP request. they just didn't want to pay for another machine...medical rationing at it's finest IMHO .Wulfman wrote:I've seen this scenario mentioned before, but it doesn't make sense to me. The insurance provider is going to pay EXACTLY the same amount of money to the DME regardless of which CPAP is given to the patient. It's the SAME insurance code. So, HOW would the insurance provider "win"? (what are they winning?)
A few years back, I made the argument that the manufacturers should ONLY make APAPs (for the CPAP category). They all have too many models that they're putting out and they all have differences inside the cases. If they only made ONE model, it would cut their manufacturing costs, big time. That model would be a data-capable APAP.......which (of course) could be set to either CPAP or APAP mode. And, the software should also be included with the machines.
Den
_________________
| Mask: Mirage Quattro™ Full Face CPAP Mask with Headgear |
| Additional Comments: 14/8.4,PS=4, UMFF, 02@2L, |
"Do or Do Not-There Is No Try"-"Yoda"
"We are what we repeatedly do,so excellence
is not an act but a habit"-"Aristotle"
DEAR HUBBY BEGAN CPAP 9/2/08
"We are what we repeatedly do,so excellence
is not an act but a habit"-"Aristotle"
DEAR HUBBY BEGAN CPAP 9/2/08
-
timbalionguy

- Posts: 888
- Joined: Mon Apr 27, 2009 8:31 pm
- Location: Reno, NV
Re: APAP, should you hit max range (now w/report)
I would like to see more 'everything in one' machines, so you would only have to buy one machine. There is an 'everything' machine now, the 'Respironics BiPAP SV Advanced. It can do everything from straight CPAP to servo veltilation. Despite its capabilities and advantages it is 1.) very expensive, 2.) only available with a prescription for a servo veltilator class machine.
I see your AHI is higher at 12 cm. This could very likely be that you have some events that there isn't enough pressure available to correct. I would consider raising your top pressure by 1 cm. Then, monitor your therapy for a while. If youe AHI goes down and/or you stop maxing out, good. Raise it another cm in a week or two if it still is maxing out. If it still maxes out, maybe your lower pressure is too low. You can leave your high end set higher if you want. But if you are seeing no improvement with your low end higher, go back to your original low end pressure. In the meantime, try to deal with as moany non-CPAP issues as you can to improve your sleep.
You will notice a 'therapy flag' line on your results labeled 'NR' for 'Non Responding'. You have no events listed there. This is where you will see what the machine thinks are central apneas reported. Seeing occasional NR events is perfectly normal. Even healthy people occasionally have centrals. It is also quite possible that the machine is reporting non-apnneic events as 'NR' eventa. LIke obstructive apneas, central apneas are normal up to 5 per hour. Above that level, it is treated with a number of things, including the servo ventilator machines.
As you raise your pressures (especially your lower pressure), keep an eye out for NR events. A few of them on the night you adjust pressure is not at all unusual. Nor are occasional NR events at any time. I have 1-3 a night, typically. But if you are suddenly seeing a lot of them, especially in clusters, back off on the pressure.
Occasional central apneas are not going to kill you at the levels most hosers experience them!
Also, be gradual with changes. What you see the first night, or even the first few nights, is not necessarily indicative of what you will see long-term. I think 4 days is the minimum to stick with a change unless it has dramatic effects. A week is better.
I see your AHI is higher at 12 cm. This could very likely be that you have some events that there isn't enough pressure available to correct. I would consider raising your top pressure by 1 cm. Then, monitor your therapy for a while. If youe AHI goes down and/or you stop maxing out, good. Raise it another cm in a week or two if it still is maxing out. If it still maxes out, maybe your lower pressure is too low. You can leave your high end set higher if you want. But if you are seeing no improvement with your low end higher, go back to your original low end pressure. In the meantime, try to deal with as moany non-CPAP issues as you can to improve your sleep.
You will notice a 'therapy flag' line on your results labeled 'NR' for 'Non Responding'. You have no events listed there. This is where you will see what the machine thinks are central apneas reported. Seeing occasional NR events is perfectly normal. Even healthy people occasionally have centrals. It is also quite possible that the machine is reporting non-apnneic events as 'NR' eventa. LIke obstructive apneas, central apneas are normal up to 5 per hour. Above that level, it is treated with a number of things, including the servo ventilator machines.
As you raise your pressures (especially your lower pressure), keep an eye out for NR events. A few of them on the night you adjust pressure is not at all unusual. Nor are occasional NR events at any time. I have 1-3 a night, typically. But if you are suddenly seeing a lot of them, especially in clusters, back off on the pressure.
Occasional central apneas are not going to kill you at the levels most hosers experience them!
Also, be gradual with changes. What you see the first night, or even the first few nights, is not necessarily indicative of what you will see long-term. I think 4 days is the minimum to stick with a change unless it has dramatic effects. A week is better.
Lions can and do snore....

Re: APAP, should you hit max range (now w/report)
NO NO NO. That higher AHI at 12 is a statistical artifact. A direct result of the very short time spent at 12 -- it should be ignored. It is all of a single apnea, happening during all of 6.9% of the night spent at 12.timbalionguy wrote: I see your AHI is higher at 12 cm. This could very likely be that you have some events that there isn't enough pressure available to correct. I would consider raising your top pressure by 1 cm. Then, monitor your therapy for a while.
AHI calculated for that proportion of time is meaningless and misleading.And you have no reason to either fear pressure induced apnea, nor to raise the top pressure.
The Respironics algorithm raises pressure like that when searching for improved results.

_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: Machine: Resmed AirSense10 for Her with Climateline heated hose ; alternating masks. |
And now here is my secret, a very simple secret; it is only with the heart that one can see rightly, what is essential is invisible to the eye.
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023

Re: APAP, should you hit max range (now w/report)
Let me see if I understand this. The therapy pressure is decreasing when a flow limitation occurs, the machine raises the pressure (solid green line), senses no improvement, raises it again, senses no improvement then drops to the last pressure (dashed green line), senses no improvement, increases the pressure again but this time to the max, senses no improvement then reduces to the original therapy pressure...right? Lotta changes.ozij wrote:..The Respironics algorithm raises pressure like that when searching for improved results.
ResMed S9 range 9.8-17, RespCare Hybrid FFM
Never, never, never, never say never.
Never, never, never, never say never.
Re: APAP, should you hit max range (now w/report)
Muse thanks for asking..I was going to.
This is getting interesting
So if I raised pressure to 13 or 14 my machine will still spike to those levels?ozij wrote:..
The Respironics algorithm raises pressure like that when searching for improved results.
This is getting interesting
Re: APAP, should you hit max range (now w/report)
One way to find out.......Imacpaper wrote:Muse thanks for asking..I was going to.
So if I raised pressure to 13 or 14 my machine will still spike to those levels?ozij wrote:..
The Respironics algorithm raises pressure like that when searching for improved results.
This is getting interesting
Den
(5) REMstar Autos w/C-Flex & (6) REMstar Pro 2 CPAPs w/C-Flex - Pressure Setting = 14 cm.
"Passover" Humidification - ResMed Ultra Mirage FF - Encore Pro w/Card Reader & MyEncore software - Chiroflow pillow
User since 05/14/05
"Passover" Humidification - ResMed Ultra Mirage FF - Encore Pro w/Card Reader & MyEncore software - Chiroflow pillow
User since 05/14/05