






I pulled a muscle in my back while bending over; fortunately, this isn't a common occurrence, having happened maybe 2-3 times in the last 15 years. Like those others, nothing terribly severe and it's close to clearing up after 48 hours, but those of you familiar with acute lower back pain know about how it initially cripples you since the back muscles connect pretty much everything else. It's hard to have any sort of range of motion when you're in blinding pain if you move your torso so much as a millimeter from being straight up and down. This presents major problems while sleeping, where if your legs aren't lined up you create some pretty intense moments merely turning. So, for the first night I knew I was going to need to medicate fairly heavily to get anything resembling sleep.
I called my PCP to double check that my treatment plan of stretching, icing, heating, and resting was correct, and then threw out my idea of a suggestion. "I'm using NSAIDs (Advil) for the day because I need to be unimpaired, but I have some hydrocodone (Vicodin) sitting around and am going to use it before bed along with a zolpidem (Ambien). I'll crank up the pressure a bit on the BiPAP to offset the CNS effects, because I doubt I'm going to get anything resembling sleep otherwise especially since I'm more than likely going to be on my back the entire night." (His response: "Try not to blow out your lungs, but as long as you don't try this more than a few days in a row that's fine, and it sounds minor enough so that you won't need to.")
By themselves, at normal dosages over a short period of time the non-benzodiazepines (Ambien, Lunesta, Rozerem, Sonata) don't affect sleep architecture. However, when combined with anything that does (like Vicodin or alcohol), they have an exponential effect. Here's your illustration of why you have to be VERY careful.
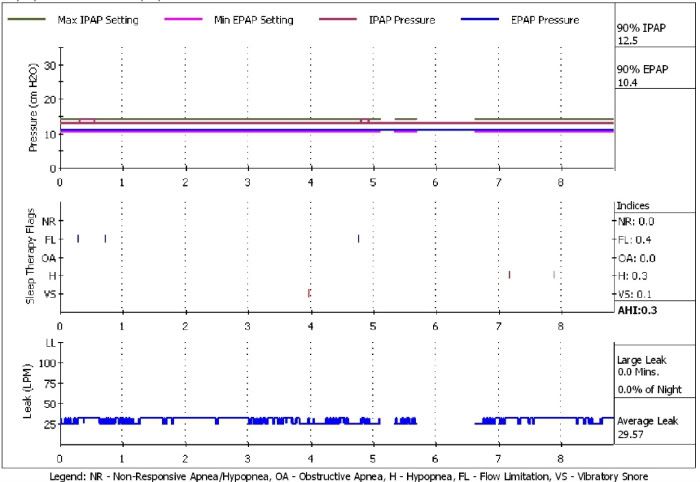
This was my sleep the night before. BiPAP in auto mode, 10.5 EPAP, maximum 14 IPAP. A typical good night for me, although I've toyed with increasing EPAP slightly for the occasional "bad" (>2.5 AHI) nights where I'm likely on my back a lot more than normal.
So, I decided that a slight increase to offset the CNS effects would be in order. EPAP went to 12, and I figured a point over my max IPAP should do it since that's been my experience when I've had a few drinks, so fixed it at 15 for a little safety margin.
Felt fine the next morning if quite stiff getting out of bed. Then I opened up Encore Pro...and went whoa nellie.
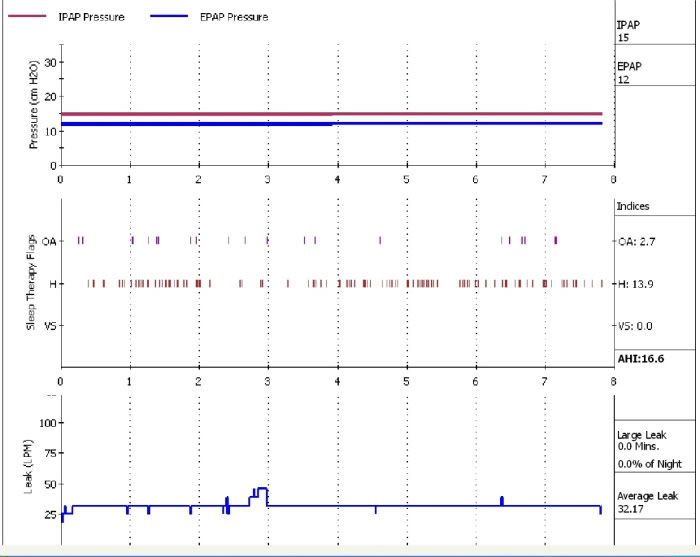
Yep. From 0.3 to 16.6 AHI. The apneas weren't horrid if not satisfactory, but that definitely breaks my all time record for hypopneas!
So last night, I let the machine work on auto mode again. 12.5 base EPAP, maximum 17 IPAP. Woke up feeling a little less rested but less stiff than I had the night before.
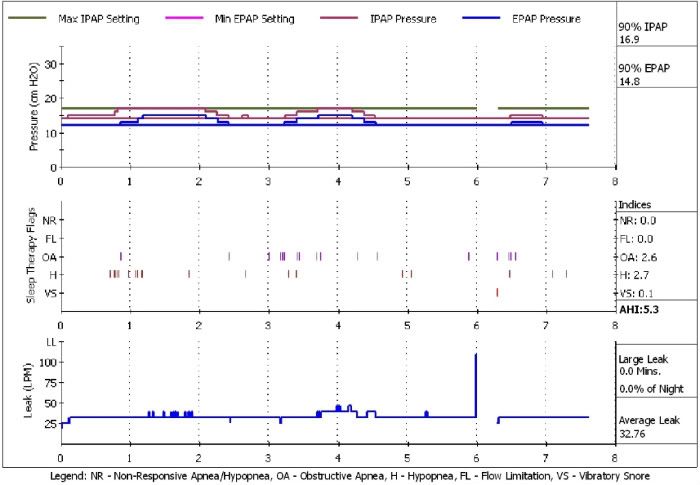
On the second night, I also used my pulse ox to monitor how severe the apneas were, and on a couple of them there were definitely desats.
The back is feeling good enough so that I'm not going to be continuing this experiment tonight, but moral of the story - be careful with anything that is a CNS depressant and be VERY careful with anything that might be additive to it. Happy Thanksgiving all.